Not sure if this is chicken or tuna salad with walnuts and grapes
Periodically there are outbreaks of illness caused by eating contaminated leafy greens. The contaminants are usually bacteria such as E coli and Salmonella. The illness is typically diarrhea, sometimes with belly cramps, nausea, and vomiting. And rare deaths.
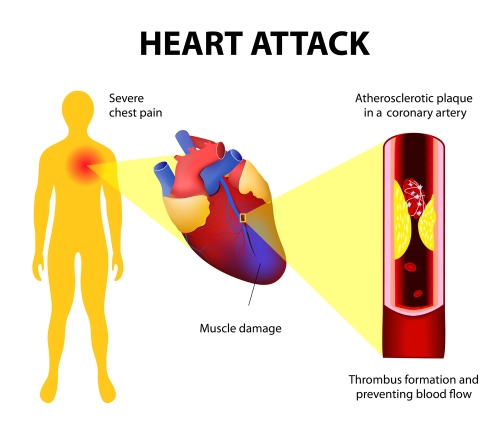
Heart attacks and chest pains are linked to blocked arteries in the heart
We’re all gonna die of something.
The #1 cause of death in the U.S. is coronary artery disease (CAD), which causes heart attacks, sudden cardiac death, and many cases of congestive heart failure. Folks with diabetes have a higher-than-average risk of CAD. Blockage in the heart arteries typically develops over years and many people are walking around not knowing it’s there. The lucky ones develop warning signs like transient chest pain or shortness of breath on exertion. After consulting a physician, the next step may be a “stress test” or some sort or imaging of the arteries of the heart.
Angiography refers to imaging of arteries or veins. Angiography of the heart arteries is helpful in diagnosing blockage of arteries that may cause heart attacks or sudden cardiac death in the future.
CT stands for computerized tomography: x-rays obtain images that are then manipulated by computer technology to provide more information than plain x-ray technology alone. CT angiography of the heart arteries is done with iodinated contrast injected into the low-pressure venous system of circulation. In contrast, standard arterial angiography involves introduction of a needle (and catheter) into the high-pressure arterial system, usually the femoral artery in the groin or the smaller radial artery in the wrist. Standard arterial angiography is associated with a higher risk of complications such as leakage of blood from the artery. Another potential complication is embolization of arterial plaque or clots downstream from the arterial puncture. Because of the higher complication rate in the arterial system, standard angiography is considered “invasive.”
Among patients referred for invasive coronary angiography (ICA) because of stable chest pain and intermediate pretest probability of coronary artery disease, the risk of major adverse cardiovascular events was similar in the CT group and the ICA group. The frequency of major procedure-related complications was lower with an initial CT strategy.
I bet the non-invasive CT is also less expensive than standard arterial angiography.
Steve Parker, M.D.
PS: Reduce your risk of CAD by controlling blood sugar, losing excess weight, exercising and heating healthy. Let me help.
From the U.S. Food and Drug Administration May 13, 2022:
Today, the U.S. Food and Drug Administration approved Mounjaro (tirzepatide) injection to improve blood sugar control in adults with type 2 diabetes, as an addition to diet and exercise. Mounjaro was effective at improving blood sugar and was more effective than the other diabetes therapies with which it was compared in clinical studies.
“Given the challenges many patients experience in achieving their target blood sugar goals, today’s approval of Mounjaro is an important advance in the treatment of type 2 diabetes,” said Patrick Archdeacon, M.D., associate director of the Division of Diabetes, Lipid Disorders, and Obesity in the FDA’s Center for Drug Evaluation and Research.
Type 2 diabetes, the most common form of diabetes, is a chronic and progressive condition in which the body does not make or use insulin normally, leading to high levels of glucose (sugar) in the blood. More than 30 million Americans have type 2 diabetes. Despite the availability of many medications to treat diabetes, many patients do not achieve the recommended blood sugar goals.
Glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) are hormones involved in blood sugar control. Mounjaro is a first-in-class medicine that activates both the GLP-1 and GIP receptors, which leads to improved blood sugar control. Mounjaro is administered by injection under the skin once weekly, with the dose adjusted as tolerated to meet blood sugar goals.
Three different doses of Mounjaro (5 milligrams, 10 milligrams and 15 milligrams) were evaluated in five clinical trials as either a stand-alone therapy or as an add-on to other diabetes medicines. The efficacy of Mounjaro was compared to placebo, a GLP-1 receptor agonist (semaglutide) and two long-acting insulin analogs.
On average, patients randomized to receive the maximum recommended dose of Mounjaro (15 milligrams) had lowering of their hemoglobin A1c (HbA1c) level (a measure of blood sugar control) by 1.6% more than placebo when used as stand-alone therapy, and 1.5% more than placebo when used in combination with a long-acting insulin. In trials comparing Mounjaro to other diabetes medications, patients who received the maximum recommended dose of Mounjaro had lowering of their HbA1c by 0.5% more than semaglutide, 0.9% more than insulin degludec and 1.0% more than insulin glargine.
Obesity was common among study participants, with an average body mass index of 32 to 34 kilograms/height in meters squared reported at the time of enrollment. Among patients randomized to the maximum recommended dose, the average weight loss with Mounjaro was 15 pounds more than placebo when neither were used with insulin and 23 pounds more than placebo when both were used with insulin. The average weight loss with the maximum recommended dose of Mounjaro was 12 pounds more than semaglutide, 29 pounds more than insulin degludec and 27 pounds more than insulin glargine. Those patients receiving insulin without Mounjaro tended to gain weight during the study.
Mounjaro can cause nausea, vomiting, diarrhea, decreased appetite, constipation, upper abdominal discomfort and abdominal pain.
Mounjaro causes thyroid C-cell tumors in rats. It is unknown whether Mounjaro causes such tumors, including medullary thyroid cancer, in humans. Mounjaro should not be used in patients with a personal or family history of medullary thyroid cancer or in patients with Multiple Endocrine Neoplasia syndrome type 2.
Mounjaro has not been studied in patients with a history of pancreas inflammation (pancreatitis), and it is not indicated for use in patients with type 1 diabetes.
Mounjaro received priority review designation for this indication. A priority review designation directs overall attention and resources to the evaluation of applications for drugs that, if approved, would be significant improvements in the safety or effectiveness of the treatment, diagnosis or prevention of serious conditions.
The starting dose is 2.5 mg subcutaneously once weekly. After four weeks dose can be increased to 5 mg once weekly. Dose can be increased every four weeks to a maximum of 15 mg once weekly.
I found a recent study involving the paleo diet at Clinical Nutrition ESPEN. I’m not paying for access to the full-text article until my book sales pick up. Access typically requires $30 USD.
The Iranian study at hand divided 80 folks into four different diet groups, to follow the prescribe diet for 10 weeks.
The Paleolithic low-carb diet “is defined as a diet consisting of 25-30% of energy from carbohydrate, 30% of energy from protein and 40-45% of energy from fat and encourages consumption of fruits, vegetables and lean meat.” There were two paleo diets: one involved calorie counting, the other portion control. All study subjects had metabolic syndrome.
This this is a mess already. And the experimental groups are tiny (20 subjects each). All diets were carbohydrate-restricted.
Results: A total of 69 participants aged 42.95 (9.27) with metabolic syndrome completed the trial. At the end of current 10-week dietary intervention trial, significant reduction in weight, waist circumference, body fat, visceral fat and waist-hip ratio (WHR) was observed in all four intervention arms (P < 0.001). Also, the observed differences among groups did not reach statistical significance (P > 0.05). Moreover, we found significant reduction in CTRP6 and leptin in all intervention groups (P < 0.001). Reduction of Asprosin level was also marginally significant between intervention groups (P < 0.05). All four intervention groups were found to improve cardiometabolic markers such as FBS [fasting blood sugar], TG [triglycerides], total cholesterol and LDL cholesterol compared to baseline. However, despite clinically significant difference, the within- and between-group changes were not statistically significant at the end of trial.
Conclusions: The current RCT [randomized controlled trial] in Iranian adults with metabolic syndrome revealed that both moderate and Paleolithic-based low carbohydrate diets with both delivery approaches have comparable beneficial effects in terms of body weight and composition, cardiometabolic factors and metabolism-related adipokines and hepatokines.
Abstract doesn’t mention calories provided (or recommended) the the four experimental diets! C’mon, man! In general, metabolic syndrome numbers improve short-term with sufficient caloric restriction regardless of the composition of the diet. E.g., eating nothing but water for five days will improve the metabolic syndrome numbers. But that’s no way to live.
I don’t know what to make of this study. But the eight researchers will undoubtedly put this article on their CVs.
Posted onMay 26, 2022|Comments Off on Recipe: Japanese-Style Avocado and Salmon Salad
If image owner (who?) objects to me posting the image, let me know and I’ll delete it.
This looks and sounds intriguing but I haven’t tried it yet. I’ve never combined avocado and salmon in an entree. I never imagined I’d like avocado in chicken soup, but it’s become a Parker Compound favorite.
Most colorectal cancers start as a growth on the inner lining of the colon or rectum. These growths are called polyps.
Some types of polyps can change into cancer over time (usually many years), but not all polyps become cancer. The chance of a polyp turning into cancer depends on the type of polyp it is. There are different types of polyps.
Adenomatous polyps (adenomas): These polyps sometimes change into cancer. Because of this, adenomas are called a pre-cancerous condition. The 3 types of adenomas are tubular, villous, and tubulovillous.
Hyperplastic polyps and inflammatory polyps: These polyps are more common, but in general they are not pre-cancerous. Some people with large (more than 1cm) hyperplastic polyps might need colorectal cancer screening with colonoscopy more often.
Sessile serrated polyps (SSP) and traditional serrated adenomas (TSA): These polyps are often treated like adenomas because they have a higher risk of colorectal cancer.
A recent study suggests that the paleo diet may lower risk of colorectal cancer. I haven’t read the full study report. Are we changing the “paleo diet” to “evolutionary-concordance diet and lifestyle pattern”? ECDLP? I don’t think so.
Abstract
Differences in diet and lifestyle relative to those of our Paleolithic-era ancestors may explain current high incidences of chronic diseases, including colorectal cancer (CRC), in Westernized countries. Previously reported evolutionary-concordance diet and lifestyle pattern scores, reflecting closeness of diet and lifestyle patterns to those of Paleolithic-era humans, were associated with lower CRC incidence. Separate and joint associations of the scores with colorectal adenoma among men and women are unknown. To address this, we pooled data from three case-control studies of incident, sporadic colorectal adenomas (n = 771 cases, 1,990 controls), used participants’ responses to food frequency and lifestyle questionnaires to calculate evolutionary-concordance diet and lifestyle pattern scores, and estimated the scores’ associations with adenomas using multivariable unconditional logistic regression. The multivariable-adjusted odds ratios comparing those in the highest relative to the lowest diet and lifestyle score quintiles were 0.84 (95% confidence interval [CI] 0.62, 1.12; Ptrend:0.03) and 0.41 (95% CI 0.29, 0.59; Ptrend:<0.0001), respectively. The inverse associations were stronger for high-risk adenomas, and among those with both high relative to those with both low diet and lifestyle scores. These results suggest that more evolutionary-concordant diet and lifestyle patterns, separately and jointly, may be associated with lower risk for incident, sporadic colorectal adenoma.
A review article in American Journal of Medicine looks at various diets that may have influence on development or progression of cardiovascular disease. All I have is the abstract, which mentions the Paleolithic diet. I don’t have access to the full article. If you do, please leave a comment below regarding the authors’ thoughts on the paleo diet. Among the 25 authors, I recognized three names; two of which are committed vegetarians or vegans (Ornish and Barnard). I suspect the article will be anti-meat.
Abstract
In cardiology clinic visits, the discussion of optimal dietary patterns for prevention and management of cardiovascular disease is usually very limited. Herein, we explore the benefits and risks of various dietary patterns, including intermittent fasting, low carbohydrate, Paleolithic, whole food plant-based diet, and Mediterranean dietary patterns within the context of cardiovascular disease to empower clinicians with the evidence and information they need to maximally benefit their patients.
My little corner of teh innerwebs here made it onto Feedspot’s Top 80 Paleo Diet Blogs and Websites list. I need to peruse some of the other sites listed when time allows. You might wanna check it out, too.
In your ideal world, would you prefer your physician’s income reflect:
number of patients seen and procedures performed, or
high quality of care, reflected in ready accessibility, lowering cost without compromising care, compliance with science-based guidelines, and patient satisfaction/experience, or
combination of the above
In other words, do you want your physician incentivized by volume or value?
The study results suggest that despite growth in value-based payment arrangements from payers, health systems currently incentivize physicians to maximize volume, thereby maximizing health system revenues.
This in-depth multimodal cross-sectional assessment of compensation and incentives among health system–affiliated POs [physician organizations] for which there is greater exposure to VBP [value-based payment] and APM [alternative payment model] arrangements compared with independent practices found that volume was the most common form of base compensation by a wide margin, being included by more than 80% and 90% of POs for PCPs [primary care physicians] and specialists, respectively, and representing more than two-thirds of compensation when included. Similarly, actions to increase volume were the most commonly cited means for physicians to increase their compensation. Base compensation incentives for physicians were not dominated by population or value-oriented payments, with only a third of POs reporting inclusion of capitation with PCPs and averaging only about a third of total compensation when included. Performance-based financial incentives for value-oriented goals, such as clinical quality, cost, patient experience, and access, were commonly included in compensation but represented a small fraction of total compensation for PCPs and specialists in health systems, operating at the margins to affect physician behavior. Taken together, these findings suggest that despite growth in APMs and VBP arrangements, these value-based incentives were not commonly translated into health system physician compensation, which was dominated by volume-oriented incentives.
The problem is that it’s a lot easier to measure volume than value. Easy wins.
Question Is cataract extraction associated with reduced risk of developing dementia?
Findings In this cohort study assessing 3038 adults 65 years of age or older with cataract enrolled in the Adult Changes in Thought study, participants who underwent cataract extraction had lower risk of developing dementia than those who did not have cataract surgery after controlling for numerous additional risks. In comparison, risk of dementia did not differ between participants who did or did not undergo glaucoma surgery, which does not restore vision.
Meaning This study suggests that cataract extraction is associated with lower risk [~30% less] of developing dementia among older adults.
Importance Visual function is important for older adults. Interventions to preserve vision, such as cataract extraction, may modify dementia risk.
Details in the abstract:
Objective To determine whether cataract extraction is associated with reduced risk of dementia among older adults.
Design, Setting, and Participants This prospective, longitudinal cohort study analyzed data from the Adult Changes in Thought study, an ongoing, population-based cohort of randomly selected, cognitively normal members of Kaiser Permanente Washington. Study participants were 65 years of age or older and dementia free at enrollment and were followed up biennially until incident dementia (all-cause, Alzheimer disease, or Alzheimer disease and related dementia). Only participants who had a diagnosis of cataract or glaucoma before enrollment or during follow-up were included in the analyses (ie, a total of 3038 participants). Data used in the analyses were collected from 1994 through September 30, 2018, and all data were analyzed from April 6, 2019, to September 15, 2021.
Exposures The primary exposure of interest was cataract extraction. Data on diagnosis of cataract or glaucoma and exposure to surgery were extracted from electronic medical records. Extensive lists of dementia-related risk factors and health-related variables were obtained from study visit data and electronic medical records.
Main Outcomes and Measures The primary outcome was dementia as defined by Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) criteria. Multivariate Cox proportional hazards regression analyses were conducted with the primary outcome. To address potential healthy patient bias, weighted marginal structural models incorporating the probability of surgery were used and the association of dementia with glaucoma surgery, which does not restore vision, was evaluated.
Results In total, 3038 participants were included (mean [SD] age at first cataract diagnosis, 74.4 (6.2) years; 1800 women (59%) and 1238 men (41%); and 2752 (91%) self-reported White race). Based on 23 554 person-years of follow-up, cataract extraction was associated with significantly reduced risk (hazard ratio, 0.71; 95% CI, 0.62-0.83; P < .001) of dementia compared with participants without surgery after controlling for years of education, self-reported White race, and smoking history and stratifying by apolipoprotein E genotype, sex, and age group at cataract diagnosis. Similar results were obtained in marginal structural models after adjusting for an extensive list of potential confounders. Glaucoma surgery did not have a significant association with dementia risk (hazard ratio, 1.08; 95% CI, 0.75-1.56; P = .68). Similar results were found with the development of Alzheimer disease dementia.
Conclusions and Relevance This cohort study found that cataract extraction was significantly associated with lower risk of dementia development. If validated in future studies, cataract surgery may have clinical relevance in older adults at risk of developing dementia.